This exercise program is not medical advice
Talk to your healthcare team about starting an exercise program before you begin.
This website should not be relied upon or serve as a replacement for medical advice from your healthcare team. Do not disregard or delay or discontinue your ongoing medical treatment because of your use of this website. Your continued treatment by your qualified medical practitioners is important to your health. If you have any concerns, address these with your medical team.
Any medical guidelines or recommendations from your medical practitioner regarding exercise in liver disease supersedes any information on this website. The information on the website is provided on an “as is” basis without any representations or warranties.
No equipment, can be done while lying or reclining in bed or on a couch, suitable for most people with cirrhosis.
Aerobic
Begin by including 5 minutes of aerobic activity on 4 days each week. For example, take a walk down the street or in a local mall. If you need to, take short rests (1 minute) either standing still or sitting down.
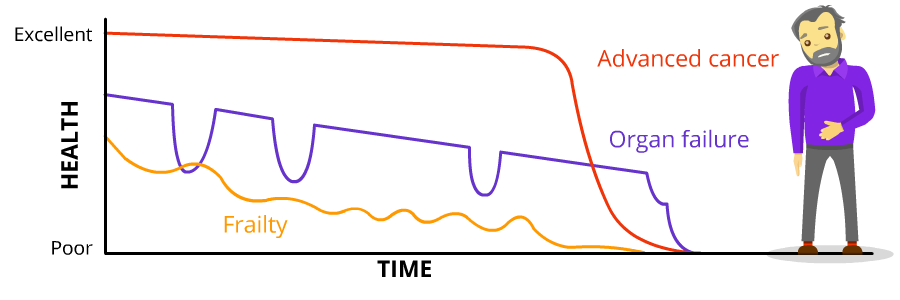
The goal is to reach and maintain between 3 to 5 on the Borg Scale – breathing stronger but can still carry on a conversation. If you reach 6 or higher on the Borg Scale, take a rest, then resume the activity.
Once you can complete 5 minutes of continuous aerobic activity, increase the session by 1 to 2 minutes.
Remember to listen to your body and take rests if necessary or decrease the duration.
Other examples of aerobic activity are: swimming, cycling, curling, lawn bowling, dancing, cleaning the garage, mowing the lawn, shoveling snow, and washing the car. Any activity can be “aerobic exercise” providing that the heart rate and breathing are increased.
Muscle strengthening
Resistance exercises improve muscle condition and strength. These exercises target muscle groups in the upper, lower, and middle (torso) of the body.
Each week, do 2 sessions separated by a few days, such as Tuesday & Friday or Thursday & Saturday.
- Each session should include 3 exercises, with 1 exercise for each body segment: upper, lower, and middle.
- Select different upper and lower body exercises for each session so that all muscle groups are similarly improved.
- For each exercise, start with 2 sets of 10 repetitions each. Gradually increase to 3 sets of 15 repetitions.
Once this is achieved, progress to 4 exercises per session.
During this session, aim to reach and maintain levels 3 & 5 on the Borg Scale – breathing moderately but can still talk.
Lateral Arm Raises
(upper body)
Arm Curls
(upper body)
Seated Triceps Extension (without banding)
For Intro level, perform this without using resistance banding. (upper body)
Seated Leg Extensions
(lower body)
Standing Leg Curls
For the Intro level, this can be performed without the resistance banding. (lower body)
Seated Calf Raises
This can be done either seated or lying down. (lower body)
Chair Sit-to-Stand
(middle or torso)
Flexibility
Start with 1 set of 3 repetitions. Hold each stretch for roughly 20 seconds or until you count to 20..
- “One Mississippi, two Mississippi, three Mississippi” and so on..
These should be done twice a week. Can be done after the Muscle Strengthening session, on their own, or combined with a Balance session.
Other stretches that can be performed while seated are: lateral side bends, chest reach, and chair-sit and reach.
Shoulder Stretch
For INTRO, perform the stretch while seated.
Triceps Stretch
For the INTRO level, perform the stretch while seated. The triceps are located in the back of the upper arm between the shoulder and elbow.
Seated Hamstring Stretch
The hamstring muscles run along the back of the thigh between the hip and the knee.
Balance
Start with 1 set of 3 repetitions and these should be done twice per week.
This can be done after a Muscle Strengthening session, combined with a Flexibility session, or its own.
Slow and steady is the rule so that multiple muscle groups are involved in controlling fine, well coordinated movements.
Knee to Chin Raises
This can be modified to a sitting position. When seated and the feet flat on the floor, lift one knee up to the chest. Keep the back straight. Repeat with the other leg. Complete for the recommended number of repetitions.
Example of a weekly intro exercise program
Aerobic: At least 4 times each week, walk continuously for 5-10 minutes. Remember to take a short break if you need to catch your breath!
Muscle strengthening: On 2 different days, do 2 sets of 10 repetitions of each of the following exercises:
- Arm curls
- Seated calf raises
- Chair-sit-to-stands
Flexibility: On 2 different days, perform all stretches 2-3 times lasting 20-30 seconds on each side.
Balance: On 2 different days, perform 3 repetitions of 10 steps each.
Arm curls
Seated Calf Raises
Chair Sit-to-Stands
References:
The information on this page was developed by the Cirrhosis Care Alberta project team (physicians, nurse practitioners, registered nurses, registered dietitians, physiotherapists, pharmacists, and patient advisors).
This information is not intended to replace advice from your healthcare team. They know your medical situation best. Always follow your healthcare team’s advice.