Everyone can benefit from learning ways to manage stress. This includes people with chronic medical conditions, like cirrhosis. My Health Alberta has excellent information and videos on stress management. If you want to learn more about stress management, we recommend you access the resources by going to MyHealth.Alberta.ca or by clicking on the links below:
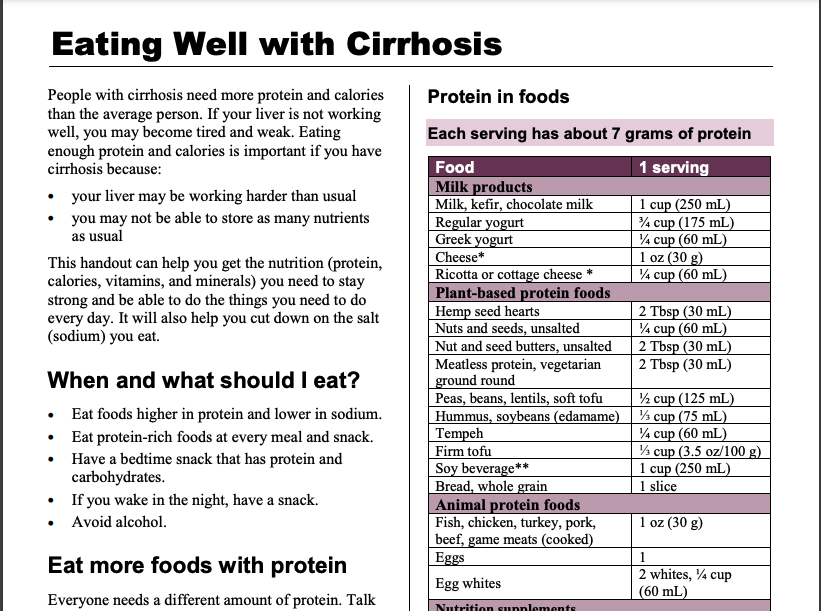
People with cirrhosis need more protein and calories than the average person. If your liver is not working well, you may become tired and weak. Eating enough protein and calories is important if you have cirrhosis because:
your liver may be working harder than usual
you may not be able to store as many nutrients as usual
The information on this page can help you get the nutrition (protein, calories, vitamins, and minerals) you need to stay strong and be able to do the things you need to do every day. It will also help you cut down on the salt (sodium) you eat.
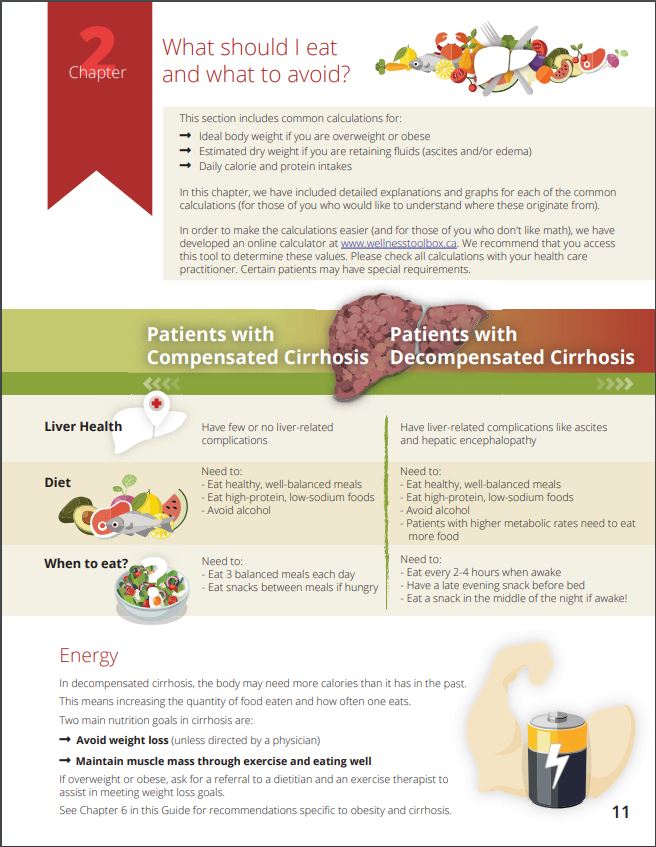
When to Eat
Some people with cirrhosis can find eating quite challenging. Lack of hunger, fluid build-up, and nausea are just some examples of things that may impact your ability to eat. You can improve your food intact by making sure you eat:
breakfast soon after you wake up
every 3 to 4 hours during the day
a snack before bed, and again if you wake in the night
Protein
Everyone needs a different amount of protein. Talk to your healthcare provider about how much is right for you. Start by eating 3 meals and 2–3 snacks each day. Have a bedtime snack every day
Protein in foods
Use the Protein in foods table below to choose:
at least 2–3 servings of protein at each meal, and
at least 1–2 servings of protein at each snack.
Protein in foods
Food
1 serving
Milk products
Milk, kefir, chocolate milk
1 cup (250 mL)
Regular yogurt
3/4 cup (175 mL)
Greek yogurt
1/4 cup (60 mL)
Cheese *
1 0z (30g)
Ricotta or cottage cheese*
1/4 cup (60 mL)
Plant-based protein foods
Hemp seed hearts
2 Tbsp (30 mL)
Nuts and seeds, unsalted
1/4 cup (60 mL)
Nut and seed butters, unsalted
2 Tbsp (30 mL)
Meatless protein, vegetarian ground round
2 Tbsp (30 mL)
Peas, beans, lentils, soft tofu
1/2 cup (125 mL)
Hummus, soybeans (edamame)
1/3 cup (75 mL)
Tempeh
1/4 cup (60 mL)
Firm tofu
1/3 cup (3.5 oz/100g)
Soy beverage**
1 cup (250 mL)
Bread, whole grain
1 slice
Animal protein foods
Fish, chicken turkey, pork, beef, game meats (cooked)
1 oz (30 g)
Eggs
1
Egg whites
2 whites, 1/4 cup (60 mL)
Nutrition supplements
Nutrition supplement drinks, bars, pudding Protein powders Protein bars, shakes
Protein amounts vary. Read nutrition Facts tables on packages.
Meals higher in protein
Add beans or lentils to soups, stews, and sauces.
Melt low salt cheese in soups, sauces, scrambled eggs, and casseroles.
Have cereal with 1 cup of milk at breakfast.
Snacks higher in protein
Add protein powder to hot cereal, smoothies, pudding, and homemade muffins.
Add unsalted nuts, seeds, and wheat germ to cereals, salads, smoothies, or yogurt.
Toast with 2 Tbsp (30 mL) peanut butter.
A muffin with cheese
Fruit and a container of Greek yogurt
A smoothie: banana, milk, protein powder.
Have a nutrition supplement drink.
Talk to your healthcare team about other ways to increase the protein in your diet.
Too much sodium can make your body hold on to extra fluid. This fluid can pool in your belly and legs. Swelling in your belly (ascites) can make you feel fuller, quicker. Eating foods with less sodium can help control ascites.
Aim to eat less than 2000 mg of sodium a day.
One teaspoon of salt has about 2300 mg of sodium.
All types of salt contain the same amount of sodium, including table salt, sea salt, and Himalayan salt.
Tips to reduce sodium:
At first, foods may taste bland. Over time, your taste buds get used to less salt.
Don’t add salt to your food while cooking or at the table.
Choose fresh, unprocessed, and homemade foods.
Eat less processed, packaged, or restaurant foods.
To boost flavours, try adding spices, seasoning mixes with no salt added, lemon, lime, vinegar, fresh or dry herbs, garlic, or onions
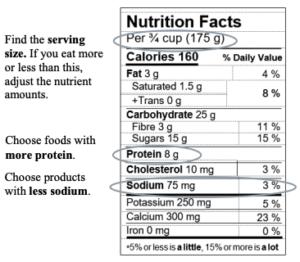
Learn to read food labels
Vitamins and Supplements
People with cirrhosis can be low in some vitamins and minerals. Osteoporosis (weak bones) is common in liver disease. Getting enough vitamin D and calcium will help keep your bones strong.
Every day, take a multivitamin and mineral pill with no iron.
You may be asked to take calcium or vitamin D pills.
Talk to your healthcare team about what kind of supplement is right for you
There are many complementary and alternative medicines that are available that claim to ease the symptoms of liver disease or to reduce your risk of developing liver disease. Most of these medicines are processed by the liver, and can be very dangerous to people with liver problems. To learn more about these medicines, Click Here.
The Importance of Nutrition to Prevent and Treat Low Muscle Mass
The Nutrition in Cirrhosis Guide
Our national team of healthcare practitioners specializing in cirrhosis developed a practical “nutrition tool” for patients. With our patients, this became “The Nutrition in Cirrhosis Guide” – intended for patients as well as their family and friends.
The Guide was made possible from extensive feedback from patients, and their family & friends, who attend The Cirrhosis Care Clinic (TCCC) at the University of Alberta in Edmonton, Alberta, Canada.
Funding for the Guide’s creation was obtained from a research grant from the Canadian Institutes of Health Research (CIHR) and Alberta Innovates. Alberta Health Services provided protected time to V DenHeyer.
The following organizations provided support in the form of unrestricted educational grants to support the Guide:
Peer review regarding the content and format of the Guide was obtained from registered dietitians (RDs) and gastroenterologists in Halifax, Montreal, Toronto, Edmonton, Calgary, and Vancouver. Additional input was obtained from experts across North America and Europe. Thank you for your valuable input and assistance.
If any portion of the Guide is used in research, communications, or patient care, please use the following citation:
Tandon P, DenHeyer V, Ismond KP, Kowalczewski J, Raman M, Eslamparast T, Bémeur C, Rose C. The Nutrition in Cirrhosis Guide. University of Alberta, Edmonton, Alberta. 2018. pp. 1- 40.
The Nutrition in Cirrhosis Guide may be reproduced for non-commercial use as is and in its entirety without further permission. Adaptations, modifications, unofficial translations, and/or commercial use of The Nutrition in Cirrhosis Guide are strictly prohibited without prior permission.
The information on this page was adapted (with permission) from the references below, by the Cirrhosis Care Alberta project team (physicians, nurse practitioners, registered nurses, registered dietitians, physiotherapists, pharmacists, and patient advisors).
This information is not intended to replace advice from your healthcare team. They know your medical situation best. Always follow your healthcare team’s advice.
Having cirrhosis can make your immune system weaker and put you at higher risk of getting sick from viruses.
Vaccines can help lower your risk.
Below you can find information about some common vaccines you can consider. Ask your health care team which vaccines are right for you and how you can access them in your community.
COVID-19
Local availability and prioritization policies will affect when you may be eligible to receive the COVID-19 vaccine. People with cirrhosis should get the first COVID vaccine they are eligible for. If you have had infection or fever, you should wait to get vaccine until you are recovered.
Until more data is available, below are some liver related COVID-19 vaccine recommendations. These are general, and may not apply to your specific health situation. Talk to your healthcare team to find out what is recommended for you.
Hepatitis B or C
If you are taking antiviral medications for Hepatitis B or C, you should NOT stop these medications while getting COVID-19 vaccines.
PBC and Autoimmune Hepatitis
If you take medication for primary biliary cholangitis (PBC) or autoimmune hepatitis, you should NOT stop these medications while getting COVID-19 vaccines.
Hepatocellular Carcinoma (HCC)
If you are being treated for HCC with ablation, embolization or chemotherapy, you should still be considered for COVID-19 vaccines without having to stop your HCC treatment
Liver Transplant Candidates
If you are waiting for liver transplant, you should get the COVID-19 vaccine, with the final dose given at least 1-2 weeks before transplant if possible.
Because liver transplant is considered a life-saving procedure, if you are offered a liver from a deceased donor, you should NOT delay your transplant because you recently received a COVID-19 vaccine.
Living Liver Donors
If you are wishing to donate part of your liver (live liver donor), you should get a COVID-19 vaccine. Your second dose should be at least two weeks before the transplant surgery if possible.
Liver Transplant Recipients
Always talk to your transplant team about COVID vaccine and your specific situation. Until more data is available, below are some considerations:
If you have received a liver transplant, COVID-19 vaccination is recommended for you.
Wait at least 1 month after transplant before getting the vaccine.
Wait at least 1-month after treatment of rejection before getting the vaccine.
If you have had COVID, wait until your symptoms are gone and you are no longer considered infectious prior to vaccination.
Wait for a period of at least 2 weeks after the administration of another vaccine.
Your anti-rejection medications should NOT be lowered for the purpose of trying to increase your immune response to the vaccine.
If you are due for a second dose of vaccine right after your transplant, the second dose can be delayed to when will likely have a better immune response.
Your household contacts should be vaccinated whenever possible.
Based on the AASLD Expert Panel Consensus Statement on Vaccines to Prevent COVID-19 Infection in Patients with Liver Disease
Influenza vaccine
If you have cirrhosis, you should get the influenza vaccine each year (usually available in the fall), to protect you against influenza viruses. This can usually be arranged through your family doctor or the public health clinic in your community. For more information, visit the links below:
If you have cirrhosis, you should get the pneumococcal vaccine to protect you against pneumococcal diseases. This can usually be arranged through your family doctor or the public health clinic in your community. For more information, visit the links below:
Hepatitis A & B are viruses that can damage your liver. If you have cirrhosis, you should get vaccines to protect you against these viruses. This can usually be arranged through your family doctor or the public health clinic in your community. For more information, visit the links below:
The information on this page was adapted (with permission) from the references below, by the Cirrhosis Care Alberta project team (physicians, nurse practitioners, registered nurses, registered dietitians, physiotherapists, pharmacists, and patient advisors).
This information is not intended to replace advice from your healthcare team. They know your medical situation best. Always follow your healthcare team’s advice.
People living with cirrhosis may not get as much exercise as they need for many reasons. Gradually, the muscles can weaken and common tasks can become more difficult to do.
Here you can start different programs in progression of difficulty, starting with the easiest.
Depending on your age and other medical conditions, your doctor might suggest a liver transplant if you’ve developed decompensated cirrhosis or liver cancer.
A liver transplant is surgery to give you a healthy liver from another person. You may get a whole new liver or just part of a new liver. The new liver may come from someone you know. Or it may come from a stranger or a person who’s died.
The waiting time for a new liver may be uncertain and stressful. The sickest patients receive highest priority. Priority is based on the severity of the liver disease as measured by a MELD (model for end-stage liver disease) score. This is simply a score calculated from four different blood tests. It helps liver transplant doctors determine which patients are at greatest danger of dying and should therefore receive transplants first.
The Procedure
A liver transplant is a major surgery that lasts 6 to 8 hours. To do the surgery, the doctor makes an incision (cut) in your upper belly. The doctor removes your liver and all its attachments. Next, they connect the blood vessels and bile duct of the new liver to your blood vessels and bile duct. The surgery is finished by closing the incision with stitches or staples. You will then be taken to the intensive care unit for close monitoring until the doctors feel you are well enough to go to the surgery unit.
After the Procedure
After a liver transplant, regular lab tests are important to check for signs of the body rejecting the new liver. Sometimes liver biopsies are also done to see if rejection is occurring. You can expect to stay in the hospital for 1 to 4 weeks and sometimes longer if there are complications. Your staples will be removed about 3 weeks after your surgery. Before you go home, your healthcare team will give you detailed information about your follow up care. You’ll need to take immune suppressing medicines and be carefully monitored for life. However, the monitoring will reduce in frequency the further out you are from your transplant.
Risks and Side Effects
People who get a liver transplant have to take drugs that suppress their immune system to prevent their body from rejecting the new liver. These drugs have their own risks and side effects, especially the risk of serious infections.
For those who had liver cancer, these drugs might allow any remaining cancer to grow faster than before. This is because the drugs suppress the immune system.
Some of the drugs used after a liver transplant can also cause:
diabetes
high blood pressure
high cholesterol
weakening of the bones and kidneys
a new cancer
Liver transplants have been hugely successful in saving the lives of patients with end-stage liver disease. Although complications may occur that will have to be managed, 85 – 90% of patients will survive the first year. Most survive to five years and beyond.
The information on this page was adapted (with permission) from the references below, by the Cirrhosis Care Alberta project team (physicians, nurse practitioners, registered nurses, registered dietitians, physiotherapists, pharmacists, and patient advisors).
This information is not intended to replace advice from your healthcare team. They know your medical situation best. Always follow your healthcare team’s advice.
Go to the nearest emergency department, or have someone call 911 if you:
are vomiting blood or something that looks like coffee grounds
have black or tar-like bowel movements
These are signs that varices may have begun to bleed.
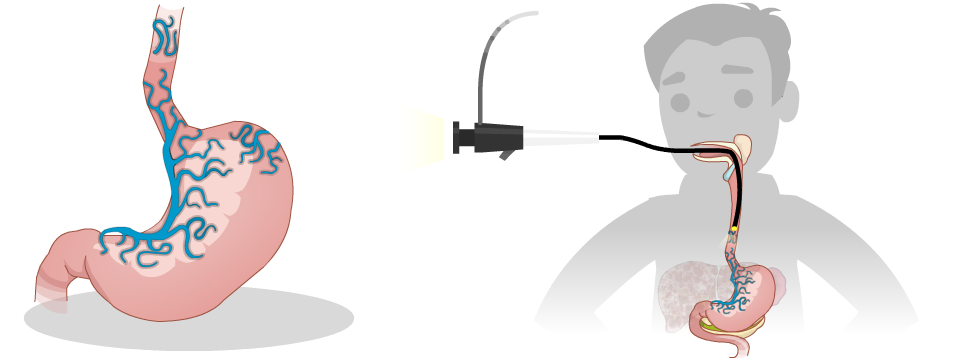
What are Varices?
When pressure in the portal vein gets too high, it can cause pressure to rise in other blood vessels. This can make the veins in your esophagus (food pipe), and stomach swell. These swollen veins are called varices. In some cases, these veins can get so swollen that they burst. This causes bleeding inside your esophagus and stomach, which is dangerous.
Symptoms
The problem with varices, is that they don’t cause symptoms until they burst open and bleed. Many people have varices and don’t know that they do. Sometimes they’re found during an upper endoscopy (also known as gastroscopy).
The more severe the liver damage and the larger the varices, the greater risk you have for bleeding varices. Bleeding varices can be a life-threatening emergency. After varices have bled once, there’s a high risk of bleeding again.
Treatment
Upper Endoscopy (Gastroscopy)
Your healthcare team will look at the results of your blood and other tests to determine your risk of having varices. If you are at higher risk, your healthcare team may want you to have a procedure called an upper endoscopy (gastroscopy). An upper endoscopy involves inserting a tiny camera through your mouth to look down into your esophagus and into your stomach. If you have varices, they can be tied off with tiny rubber bands during the procedure (called banding).
If your first upper endoscopy didn’t find any varices, you will likely have another one again in 1 to 3 years. If you have varices, you may need more frequent upper endoscopies. You’ll also need to have an upper endoscopy more often if you’ve had bleeding varices.
Medication (nonselective beta-blockers)
Your healthcare team may also prescribe blood pressure medicine called nonselective beta-blockers to help lower the risk of bleeding from varices. If you take this medicine, you’ll need to check your blood pressure and pulse regularly. If you feel dizzy, lightheaded, or fall, let your doctor or nurse know.
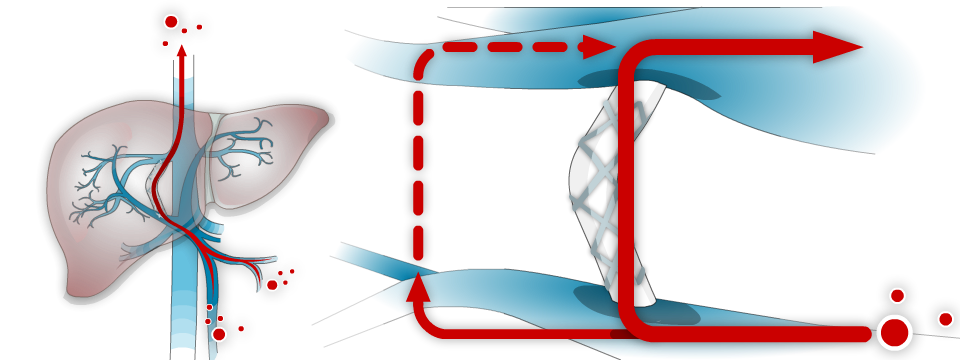
TIPS (a shunt used to decrease pressure in the portal vein)
In more severe cases, an TIPS procedure may be required to stop or prevent future bleeding. This is a procedure done by an interventional radiologist in a specialized hospital.
For more information on these treatments, please click the links below:
The information on this page was adapted (with permission) from the references below, by the Cirrhosis Care Alberta project team (physicians, nurse practitioners, registered nurses, registered dietitians, physiotherapists, pharmacists, and patient advisors).
This information is not intended to replace advice from your healthcare team. They know your medical situation best. Always follow your healthcare team’s advice.
To view this video with Spanish subtitles, Click Here.
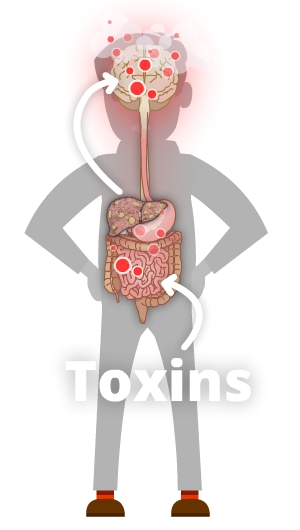
What is Hepatic Encephalopathy?
When the liver’s been damaged by cirrhosis, it might not be able to get rid of toxins such as ammonia. As a result, ammonia and other toxins may build up in your bloodstream and brain. This causes a problem called hepatic encephalopathy (pronounced “en-sef-a-lop-a-thee”). You may hear your healthcare team call it HE for short. When you have HE, toxins build up which can cause confusion and other symptoms.
Causes
Encephalopathy is most likely to occur in people who have high pressure in their portal vein (portal hypertension). It may also occur in people who have severe acute liver damage (liver damage that happens suddenly) but no portal hypertension.
Also, a procedure called TIPS that is used to lower portal hypertension by shunting blood flow around the liver can increase your risk for encephalopathy.
Other things that might contribute to encephalopathy include:
abnormal levels of electrolytes
constipation
not getting enough fluids to drink or loosing fluids too quickly (dehydration)
internal bleeding
infection
medicines like pain killers and sleeping pills
Symptoms
Symptoms of encephalopathy might include:
coma
disorientation (not remembering where you are or what’s happening)
difficulty remembering the right words to say
drowsiness
hand “flapping”
sleep pattern changes
feeling irritable
trouble concentrating
poor short-term memory
having tremors
Treatment
Your Support Network
Share what you learn about hepatic encephalopathy with your caregivers, friends, and loved ones. This is important because having encephalopathy can make it hard for you to care for yourself at times, and you may need extra support. Your support network can help you watch for emergency warning signs. For example, if they notice you’re really confused or have trouble waking up, they can call 911 or take you to the nearest emergency department.
Lactulose
In most situations, encephalopathy is treated with a medicine called lactulose. Lactulose is a laxative syrup that makes your bowels move more often and also makes your bowel movements more acidic. This helps your body to get rid of toxins like ammonia from your body.
If you are taking lactulose, you should take enough so that you are having 2 or 3 soft bowel movements each day. If you take too much you will get diarrhea, but if you don’t take enough you will develop encephalopathy symptoms. You should increase the amount you are taking if you are not having enough bowel movements. Finding the right balance for you is the key. You can get more information about lactulose (including potential side effects) from your pharmacist.
Rifaximin (Zaxine, Xifaxan)
Another treatment for encephalopathy is rifaximin. Rifaximin is an antibiotic that stays in your digestive system and changes the bacteria in your gut so they make less toxins like ammonia. Rifaximin comes as a pill and is usually taken two times a day. You can take it with or without food. You can get more information about rifaximin (including potential side effects) from your pharmacist.
Self Care Tips:
If you are being treated for hepatic encephalopathy:
Avoid medicines that can make you sleepy
Record the number of bowel movements you have each day in a notebook or app on your phone
Take enough lactulose so you have 2 to 3 medium to large, soft bowel movements a day.
Don’t take more lactulose than you need because it may make you dehydrated.
If you develop a mild increase in your encephalopathy symptoms, take more lactulose (as long as you are not having diarrhea, fever, or signs of bleeding).
Let your healthcare provider know if you:
have trouble adjusting your dose of lactulose
feel tired, sleep more, or your sleep patterns change so you’re up at night and sleep during the day
have trouble concentrating or remembering things
have a change in your personality
notice shaking of your body (called a tremor) or are unsteady (feel like you may fall)
The information on this page was adapted (with permission) from the references below, by the Cirrhosis Care Alberta project team (physicians, nurse practitioners, registered nurses, registered dietitians, physiotherapists, pharmacists, and patient advisors).
This information is not intended to replace advice from your healthcare team. They know your medical situation best. Always follow your healthcare team’s advice.

 Our national team of healthcare practitioners specializing in cirrhosis developed a practical “nutrition tool”
Our national team of healthcare practitioners specializing in cirrhosis developed a practical “nutrition tool” 













 When pressure in the portal vein gets too high, it can cause pressure to rise in other blood vessels. This can make the veins in your esophagus (food pipe), and stomach swell. These swollen veins are called varices. In some cases, these veins can get so swollen that they burst. This causes bleeding inside your esophagus and stomach, which is dangerous.
When pressure in the portal vein gets too high, it can cause pressure to rise in other blood vessels. This can make the veins in your esophagus (food pipe), and stomach swell. These swollen veins are called varices. In some cases, these veins can get so swollen that they burst. This causes bleeding inside your esophagus and stomach, which is dangerous.